Healthcare facility use of electricity is not declining: Hospital Energy and Water Benchmarking Survey 2021 from GrummanlButkus
Grumman|Butkus Associates, a firm of energy efficiency consultants and sustainable design engineers, released the results of its 2021 Hospital Energy and Water Benchmarking Survey focusing on healthcare facilities’ resource usage trends and costs for the year 2020.
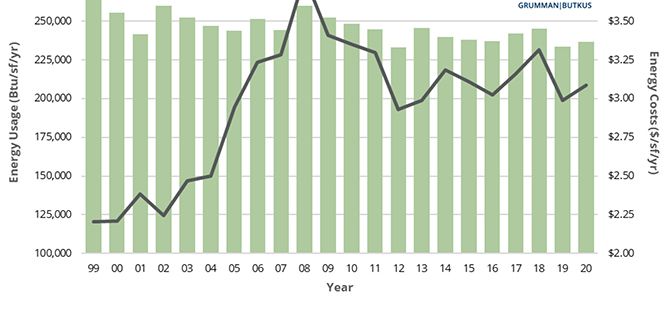
Since GBA initiated the survey more than 25 years ago, hospitals’ overall fossil fuel use has trended downward, but electricity use isn’t declining as much. The average combined Btu/ft2 (electricity plus gas/steam) for participating facilities was 236,743 in this year’s survey, up from 233,491 in CY2019. However, interpretation of year-to-year trends should be tempered by the realization that the respondent pool for the 2021 survey was different from the pool from the 2020 edition, due to the stresses that COVID-19 response placed on the healthcare facility personnel who normally participate, particularly during CY19.
Square-foot prices for gas/steam fell ($0.65 in 2020, compared with $0.67 in 2019), but square-foot prices for electricity were up ($2.44 in 2020, compared with $2.32 in 2019). The overall result is that total reported ft2 costs for energy (gas/steam plus electric) increased: $3.09 for 2020, compared with $2.99 for 2019.
Hospitals’ average carbon footprint has remained fairly steady at 50 to 60 pounds of CO2 equivalent per ft2 per year since GBA began calculating carbon data in 1999. CO2 footprint in 2020 was up from a low in 2019 (likely attributable to a change in respondents for the 2020 survey), but still shows an 18% decrease from 2018. “To meet the ambitious goals put forth by the Biden Administration, hospitals will have to achieve much more significant reductions in the near term,” says GBA-Illinois Chairman Dan Doyle. “These reductions can only be achieved by implementing larger and more costly retrofits of existing buildings. The drive to decarbonize will also require building owners to embrace fuel switching to renewable-based energy sources. Many leading healthcare systems are implementing on-site renewables (usually solar photovoltaic systems), as well as off-site renewables, often funded through Power Purchase Agreements (PPA) to purchase some or all of their electricity.”
Participating facilities displayed a broad range of energy usage patterns. For instance, a few of this year’s survey participants reported fossil fuel consumption of more than 200,000 Btu/sf/year, compared with the general mid-range of facilities (about 130,000 Btu/sf/year) and those that used the least (75,000 Btu/sf/year or less). These variations mean that hospital fossil fuel energy costs may exceed $1.50/sf/year or come in at less than $0.50/sf/year.
Similarly, several hospitals were consuming more than 40 kWh/sf/year in electrical energy, compared with a mid-range of about 27 kWh/sf/year. A few survey participants squeaked in at less than 20 kWh/sf/year. The wide differences in usage mean that some of our participants are paying well over $4.00/sf/year for electrical energy, while many are getting by at less than $2.50 and a few at less than $1.75.
“Facilities that have high unit costs for energy should view this as an opportunity,” says Doyle. “For example, a project that would have a five-year payback at an ‘average’ facility may have a payback of just 2.5 or 3 years at a facility with higher unit costs for energy.”
Hospital water/sewer use is also gradually declining, averaging about 36 gallons per square foot per year in CY2020 (compared with more than 60 gallons/ ft2/year in 2006, the year GBA began tracking water/sewer use). Costs for water/sewer are generally rising, however. The 2020 data reported by respondents, with an average annual water/sewer cost of $0.34 /ft2, represents a significant drop from 2018 but is still up slightly from 2019, and is considerably higher than the $0.27/ft2 that hospitals were spending in 2006.)
“GBA expects the general trend of rising water and sewer costs to continue,” says Doyle. “Price hikes not only reflect increasing costs to extract and treat the water, but also the expense of upgrading or replacing aging infrastructure. In addition, some cash-strapped governmental entities may view water as a revenue sources.”
Since 1995, the GBA survey has provided a free annual benchmarking resource. Hospitals are invited to participate by submitting responses to a short list of questions. Information for this edition was provided by 132 hospitals located in Illinois (48), Wisconsin (28), Indiana (16), Michigan (9), Nevada (7), California (5), Missouri (5), and numerous other states coast-to-coast.
Full results and analysis in the 2021 Hospital Energy and Water Benchmarking Survey as well as information about participating in the 2022 survey (2021 data), are available at the firm’s website. The 2021 data is important, notes the firm; it will be based on different operating conditions than in previous years. Respondents’ 2021 data will improve overall understanding of the pandemic’s continuing impact on hospital energy and water use, and increase knowledge within the healthcare community.